Should visiting a GP doctor be free or should we pay to visit the doctor? It is an emotional issue as in the UK there is a strong acceptance of free health care, but what are the economic arguments? Could we have better health care by charging people to see their GP?
Benefits of charging to see your doctor
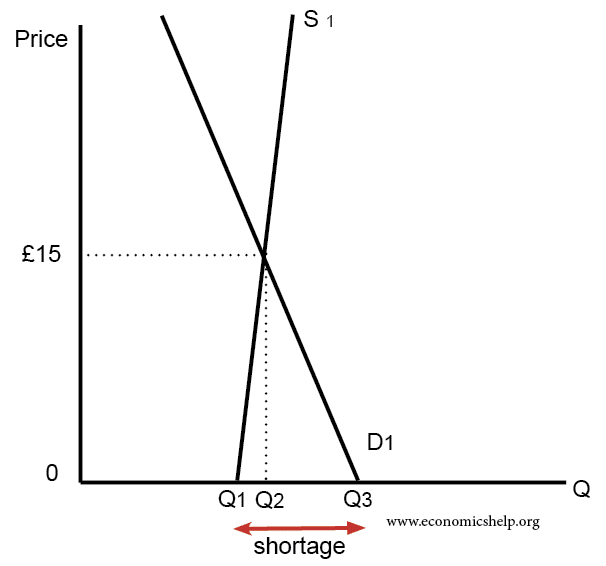 When health care is £0, demand (Q3) is greater than supply Q1. Charging £15 would cause a movement along demand curve and an expansion in supply and, in theory, end waiting lists.
When health care is £0, demand (Q3) is greater than supply Q1. Charging £15 would cause a movement along demand curve and an expansion in supply and, in theory, end waiting lists.
- Free appointments can lead to a shortage. Currently, in the UK there is a shortage of GP appointments. Demand outstrips supply and this leads to an average waiting list of over 2 weeks (link). This is frustrating for patients who need to be seen sooner.
- If it is free, people may go even if they don’t really need to. Charging for a doctor’s appointment will reduce the incentive to go for very minor issues, leaving more appointments for people who really need it.
- If people pay to see the doctor, they are more likely to turn up for their appointment. At the moment, there is no cost of missing an appointment and this leads to wasted appointments. According to NHS England “15 million general practice appointments are being wasted each year because patients do not turn up” (link) The NHS claim that the cost is £30 per missed appointment, creating a total cost to the NHS of than £216 million.
- It will raise revenue for the government which can be spent on the NHS. Most patients would feel that for the cost of £15, a better funded health service and shorter waiting times would be worth it. In England, there are 300 million GP appointments per year. Charging £15 per appointment would raise £4.5 bn (link) This would enable a very significant expansion in GP numbers and the number of available surgeries.
- It could be combined with giving patients more choice on which doctor they see.
Disadvantages of charging for the NHS
- Health is a merit good, people underestimate the benefits of going to the doctor – e.g. for cancer screening; charging would put some people off. If GPs miss early signs of cancer/ill health, it can prove more costly in the long run to treat. Therefore, these kind of health checks should be free.
- GPs are often in the position of having to advise patients to change diet, change lifestyle – e.g. stop drinking, stop smoking, cut down on sugar and lose weight. These kind of lifestyle changes can be more effective than expensive drugs. However, if patients are paying to see the GP, they may not want to pay to hear they should lose weight. Paying patients may feel they have a right to be proscribed antibiotics (even when they don’t really need them.)
- Health has positive externalities which are ignored in a free market. If you have flu, the doctor can advise you on staying home, not infecting other people. Timely treatment and advice from your GP can get you back to work quicker – this will lead to benefits for firms and the economy.
- Demand for health care is inelastic, therefore charging may not reduce waiting lists.
- It is debatable whether many people go to the GP just because it is free. There are still costs in taking time out of the day. Most people don’t go unless they have to.
- Administration costs of collecting money. Surgeries will also have to start collecting money from patients, creating more admin.
- It will also change the relationship between doctors and patients. We trust doctors are acting in our best interest, but when we start paying a doctor we have different attitude to the GP surgery.
- Charging to see the doctory would be a regressive charge. It would be a bigger percentage of income for those who are on low-income.
- It would also be a bigger share of income for those who are ill. When you are ill and not able to work, you may already be financially stretched, having to pay to see the GP would impose an additional cost.
- There are other ways to raise finance for the NHS. Rather than collecting from patients directly, the government could raise taxes (VAT or income tax). It could impose a sugar tax or higher alcohol tax to help reduce levels of obesity and alcohol-related problems.
Conclusion
This is an interesting question. Superficially, there is a good economic case for charging people to see the doctor. It is a logical response to a shortage of demand. However, we have to be careful with basic economy analysis. For example, would a charge discourage people from going to see the doctor and then end up costing the NHS more because the illness becomes more serious?
Also, it is very interesting how charging to see the doctor would change our relationship with the GP. A fee paying patient may have a subtle feeling they can demand the GP treats them in a certain way. It reminds my of the “Moral limits of markets” by Michael Sandel.
Related
I’ve worked in healthcare settings as a gp where it has been both free and also where it costs. New Zealand was one and had a charge similar to 15 pound to see your GP. It was free for children under 12, reduced cost for those between age 12-18 and also those for lower incomes. We had a set government allocation where we could also give 4 free appointments that year to any individual. This would usually be a new diabetic or new hypertension with the goal to investigate and get these conditions under control thereafter diabetes patients had a free twice yearly reviews and similarly with a few other conditions. People often self triaged to the pharmacy or our in house physiotherapist.
Home visits cost more about 35 pound. I covered a very large geographic area and to put things in context outside of the weekly visit to the nursing home I did 6 home visits in 6 months, I can often do that in a day over here as people do not value this service appropriately. Any delays in healthcare over there that I saw came more from the secondary care side of things e.g. 18 months for a knee replacement 8 weeks for a ct scan. New Zealand has a longer life expectancy than the UK and this despite very skewed figures within the Maori population which has been a challenging area to improve healthcare outcomes on.
I also had 15 minute appointments with patients. I saw 2/3rds of the normal here and had very few phone calls compared to here. I’m originally Irish and think the charge of 50 euro over in Ireland for about half the population is counter productive and almost definitely changes the relationship. But I did not find that the case in New Zealand with a similar charge of 15 pound. In fact I found it the opposite patients often engaged better with lifestyle advice when given more time to explain it etc. They would often choose this path also as medication was 5 dollars (2.50) for each item for a 3 month supply, so if something was free and could achieve better or similar outcomes e.g back exercises for back pain, weight loss for urinary stress incontinance they would often be more encouraged to take that route.
To date I have found it the best system I have worked in and I looked after a slightly bigger and very much geographically spread out population. I could easily work 5 days there but over here the intensity after 3 days one is pretty broken (and we even covered OOH’s there but with nurses doing the visits and us being available via phone, I would come in for the occasional difficult case). It was not all perfect as people due to the government accident insurance system would falsify there history to have a free appointment stating something was an accident when it wasn’t but this was pretty rare overall. We have one of the lowest doctor to patient ratio’s in the oecd I.e 2.8 per 1000 people compared to the average of 3.5 per 1000. We really do need an economic solution to this as it is breaking general practice. If supply can be markedly increased fine. However, we were promised 5000 gps extra in England 5 years ago and we are actually down 1000 FTE compared to then when the original pledge was made. So realistically Indi not see this forthcoming. The waits and queues will likely get longer.
The only way to reduce them is to use allied health professionals however even finding people to hire for this has been difficult and lots leave as the find the undifferentiated presentations of general practice very challenging and boxing people into just see the mental health nurse leaves out the holistic approach e.g maybe their depression is secondary to their poorly treated copd and fatigue and by not addressing both at the one consult we are doing a disservice to our patients. Just my 2 bits.
Thanks for interesting observations
Back in 1967 I was discharged from HM Forces due to a Serious accident, since then I have spent many years in and out of hospital. I have observed staff working: doctors, nurses cleaners etc. and all have been worked off the feet, especially over the last decade.
It is virtually impossible now in the UK to get a GP appointment and waiting lists for hospital appointments stretch from London to Timbuktu, it is a desperate situation, mainly brought brought about by poor pathetic political management.
I declare here that I am not a racist but uncontrolled immigration to the UK has placed an immense burden on the NHS.
When Aneurin Bevan introduced the NHS in 1948 the population would have been nowhere near what it is now in the Disunited Kingdom.
Taking into account the dire public spending figure of £5,170 per second, an annual figure of £163,041,120,000 , and the fact that the British economy is contracting BIG TIME, I believe that there will be introduced a fee to see a doctor, my intuition tells me it will start at £26 and will be based on ability to pay,e.g in a household where there is a joint income of £30,000 or an individual earning £30,000; no if’s or but’s it is going to happen.
I thank you for your article which I found interesting.
Best Wishes,
Desmond Whittle